Shoulder Debridement Coding: CPT 29822, 29823, and Practical Examples
By Paul Cadorette, CPC, COC, CPC-P, COSC, CASCC, Director of Education, nimble solutions
WATCH THE ANATOMY OF CODING Shoulder CODING COURSE ON DEMAND. REGISTER HERE
Shoulder debridement is a common orthopedic surgery, yet there is confusion concerning its two main codes CPT 29822 and 29823.
In this post, we’ll delve into the nuances of arthroscopic shoulder debridement, shedding light on the key aspects of the procedure and how it is coded.
CPT Codes for Shoulder Debridement: 29822 and 29823
Shoulder debridement is represented by two main codes: 29822 for limited debridement involving one or two discrete structures, and 29823 for extensive debridement involving three or more discrete structures.
The term “discrete structures” refers to specific anatomical locations, as outlined in the CPT Manual, which are as follows:
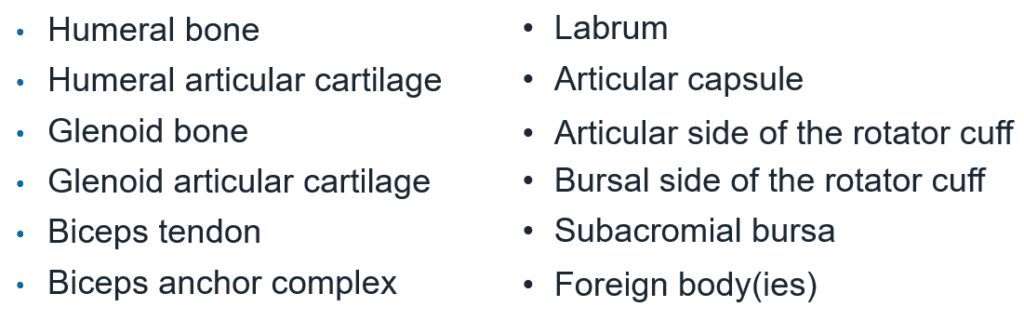
It’s crucial to note that, with the exception of foreign bodies, discrete structures are anatomical, not pathological.
For instance, synovitis and adhesions, while indicative of pathology, are not considered discrete structures. Treatment of these pathological conditions requires the use of other existing CPT codes, such as 29820 or 29821 for synovectomy and 29825 for lysis of adhesions.
Coding for Shoulder Debridement: Distinguishing Anatomical and Pathological Conditions
To properly code for shoulder debridement, it’s essential to differentiate between debridement of discrete structures (anatomical locations) and treatment of pathological conditions (e.g., synovectomy, lysis of adhesions).
Counting the number of discrete structures debrided serves as the initial step in this process.
For instance, chondromalacia is considered pathology because it affects the cartilage of bones and debridement of cartilage (humeral or glenoid), so it can be considered in your discrete structure count whereas debridement of synovitis is still considered a synovectomy and is therefore not counted.
Moreover, when a structure undergoes debridement followed by repair, only the repair code can be reported.
In such cases, the debrided structure must be subtracted from the initial debridement count. This ensures that the debridement procedure is not redundantly coded alongside the repair.
Shoulder Debridement: Practical Example
Consider a scenario where a surgeon performs debridement on the rotator cuff, labrum, and biceps tendon. Subsequently, repair procedures are carried out for a rotator cuff tear, SLAP lesion, and biceps tenodesis.
In this case, the debridement count would be zero, as all debrided structures were also repaired.
Consequently, the debridement becomes inclusive to the repair procedures and is not separately reportable.
Conclusion and Further Learning for Shoulder Debridement Coding
Understanding the nuances of shoulder debridement coding is crucial for accurate coding, billing and reimbursement for orthopedic ASCs.
If you found this information helpful, consider delving deeper into shoulder coding by attending our upcoming nimble shoulder coding course, scheduled for March 19th at 1pm Central Time.